
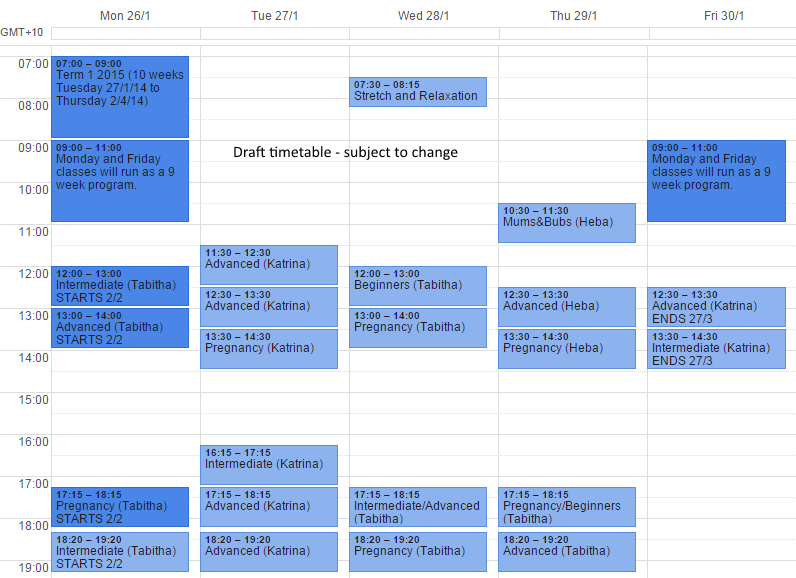
Draft Pilates Timetable Summer School 2015
12 November 2014 Pilates, Sydney CBD
Draft timetable for our $1 and $1
Read More Draft timetable for our $1 and $1
Read More
Tips on choosing the right back back Considering that 60-80% of us will experience back pain in our lifetime, choosing the correct back pack for us or our children should be a priority. The high number of children and adolescents already complaining of back pain is astounding. Studies recently in So...
Read More
Lost focus? Do you ever feel that your exercise really isn't grabbing you? Are you bored with it? Not looking forward to the next session? Making excuses to avoid exercising altogether? We are all individuals and therefore the gym/running/getting sweaty is not for us all. So we all know the well doc...
Read More
Katrina spends a day in front of the camera for 12WBT This September saw 12 Week Body Transformation launch 2 new programs – for $1. $1 has more of a reputation around working out, weight loss and adopting a positive long term outlook to well being, lifestyle and exercise. The pregnancy and post-nat...
Read More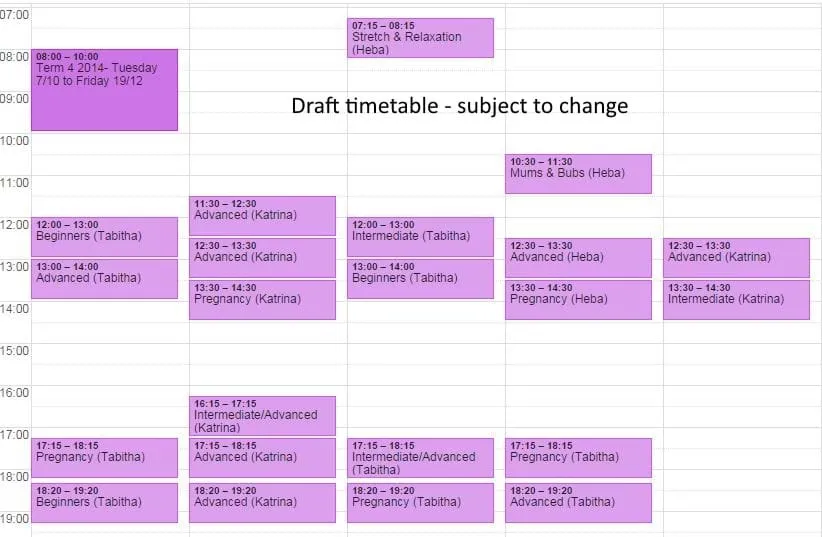
Draft timetable for our $1 and $1
Read More
Katrina shares her experience with podiatrist $1 OK, so l'm a physio and should practice what I preach. Hmmm.....well. I've got to be honest and have always been resistant to wearing orthotics, however with an increasing enjoyment for pounding the pavement, I am starting to notice that I perhaps don...
Read More
Discover what causes those "embarrassing leaks" Do you leak a little whenever you cough or sneeze or laugh? Or maybe you only leak when your bladder is full and then you cough or sneeze? Perhaps you notice some leaking during sex or when you're exercising – it may be during star jumps, jumping on th...
Read More
Exercise 'specificity' at its best $1 Watching this youtube clip showing dancers in slow motion makes you realise how perfect these skilled dancers are in their movement and movement control. What is even more interesting is how precise and targeted the strengthening exercises are to exactly target...
Read More
Podiatrist Lance Penn from Footsport guest posts An orthotic is a custom made device designed to off load abnormal forces that can lead to damage of soft tissue structures, joints and bones. **What causes injury?** The direct cause of pain is a consequence of damage to the body (muscle/tendon/ligame...
Read More
Ineffective? I say misleading. You may have recently heard in the mainstream media that there is a big question hanging over the effectiveness of Paracetamol in the management of early back pain. This was based on a very recent study by Australian team of scientists who were published in the highly...
Read MoreShowing 10 of 298 articles by Katrina Tarrant